
I’m wondering if there is something else viral / cardiac going on as well. I lost my medical for 5 weeks recently due a totally unexpected hypertensive crisis after a viral (non COVID infection) and I hear stories of record numbers of people failing medicals on BP at the moment. Tragically I heard today of a friends father who has died running at 61, a totally fit individual. This comes after someone else I knew who died running aged 64 just before Christmas.
MattL wrote:
I’m wondering if there is something else viral / cardiac going on as well. I lost my medical for 5 weeks recently due a totally unexpected hypertensive crisis after a viral (non COVID infection) and I hear stories of record numbers of people failing medicals on BP at the moment. Tragically I heard today of a friends father who has died running at 61, a totally fit individual. This comes after someone else I knew who died running aged 64 just before Christmas.
Hypertension is a “pandemic” that precedes Covid-19 by decades and is far more relevant in its overall morbidity and mortality in Western societies.
I am not aware of any virus causing it, although there might be unknown correlations. The major known risk factors are diet and lack of exercise.
A relative of mine died yesterday from a heart attack. He was scheduled for an operation in March which was cancelled due covid. He was supposed to be going in sometime in Jan.
All annecodotal but I know of a number of people who’ve died this year. Not a single one of covid.
Yes this has been a recurring topic in 2020. Quite a number of people we knew have died. None confirmed from CV19.
I think BP can be lots of things.
A lot of people are spending time “with the family” and for many this is very stressful. For example my BP might be 135/75, but if I was in the same room as my sister, or my ex, it would be 165/105 which is way too high. Solution: avoid contact (have done for some years now)  It is sadly the case that many relationships work only with long absences, and when you remove these absences, stuff just blows up.
It is sadly the case that many relationships work only with long absences, and when you remove these absences, stuff just blows up.
BP is also very much diet related. If you substantially drop meat and dairy (especially dairy) your BP will drop maybe 10/10. And I think a lot of people are eating more crap when sitting at home.
But, yeah, who knows? Maybe asymptomatic CV19 bungs up your arteries? If you have that and try running fast, you will get ischemia pretty fast. An ECG treadmill is thus highly diagnostic.
Peter wrote:
A lot of people are spending time “with the family” and for many this is very stressful. For example my BP might be 135/75, but if I was in the same room as my sister, or my ex, it would be 165/105 which is way too high. Solution: avoid contact (have done for some years now) It is sadly the case that many relationships work only with long absences, and when you remove these absences, stuff just blows up.
That has really cheered me up and made me laugh – absolute gem.
There is obviously a question to be asked about what ICU utilisation ‘should’ be in normal (non-pandemic) circumstances.
Obviously in the UK the system is almost completely nationalised. In the rest of Europe substantially so.
Given that funding model, one would perhaps hope not to see significant spare capacity most of the time, lest it be considered a waste of money?
In the US I’d imagine simple market forces take over, and the more you pay for your care (or your insurance) then the more you can reasonably expect standby capacity to be just sat there waiting for you to be admitted.
As an anecdote, in the summer of 2019 I had one of my very rare interactions with healthcare of any sort. Very severe GI disturbance, very high fever, hallucinations, lost 6kg., etc. Because my girlfriend had to travel for work for the next 3 days, she dropped me at the local hospital A&E (ER) at 6am on a Monday morning – realistically at that time of day A&E is the only part of the NHS open and accepting patients. The place was completely deserted, apart from lots of doctors and nurses, and I was seen immediately and the care was outstanding. I had mixed feelings about the whole thing – on the one hand I was delighted at the performance of the much-maligned NHS in this particular instance, and on the other hand the management account in me was getting a bit worked up about all this unused capacity sat there doing nothing and costing money!
Then again, there are Friday and Saturday nights … :-o
on the other hand the management account in me was getting a bit worked up about all this unused capacity sat there doing nothing and costing money!
You need a certain amount of spare capacity in healthcare to run efficiently. When you don’t have it, things become dangerous and inefficient. Quite what the magic number is, I don’t know – perhaps 80% or so would be about right.
When I worked in a very small emergency department we averaged 60 patients a day. That meant that 95% of the time you would expect between 45 and 77 patients a day. In practice occasionally you get none (when there is a storm and all the roads to the hospital are closed) or 120 patients when there is a local rugby tournament. Obviously you need to have a level of staffing that is safe even when the department is exceedingly busy.
Compare that to the largest hospital in the region which has 500 – you would statistically expect between 457-545 patients a day. Proportionately the variability in workload is far less, which I suspect is part of the reason there is a drive towards larger hospitals.
I remember one night when we had 6 men in a two-bedded room and in a four bedded room. There were 6 women in a seven bedder. Along comes another man who needs to be admitted. What do you do? Of course you move all the women to the rooms that the men are in and you move all the men to the room that the women are in, so that you can put the new man in a room without mixing sexes. All the rooms need to be thoroughly cleaned as the patients are moved, and it means that twelve patients don’t get any sleep that night, and everybody is busy simply cleaning and moving people around.
There are also benefits in terms of infection control in leaving rooms and operating theatres fallow for a time between patients.
It’s true that night shifts can be more relaxed than daytime shifts, but the nursing staff generally have jobs such as checking drugs cupboards and cleaning that they do when the department is quiet. Doctors have educational or governance tasks that can keep them occupied. You sound as if you were pretty unwell and it may be that some of the doctors dropped other tasks to come down to the department.
Excellent comment, @kwlf !
In healthcare, there must be lot of what we call in German Vorhaltekosten , which roughly translates as “cost of keeping (someone or something) at the ready”. Otherwise you have no spare capacity and even a single additional emergency patient overloads the system. I think kwlf’s figure of about 80% capacity usage as “optimum” sounds about right. That gives you 20% spare capacity.
The pandemic has shown – once again – that the limiting factor of capacity are usually qualified staff. Early on in the pandemic, everybody was scrambling to buy ventilators, which made my Dräger stocks rise nicely, but did almost nothing to help actual patients, because these devices need well trained staff to operate. In most western health care systems, staff is running near or at 100% of their capacity at most of the time. There is very little staff reserve, if any. In many countries, the military had to help out, and they don’t exactly have tons of medical staff doing nothing otherwise either (at least in Germany, the Bundeswehr is always looking for doctors and paramedics. They even rose the age limit of hiring doctors to 62 (!), which led to my father – who never did any previous military service – joining as a reserve officer at the rank of Major last year – he’s 59).
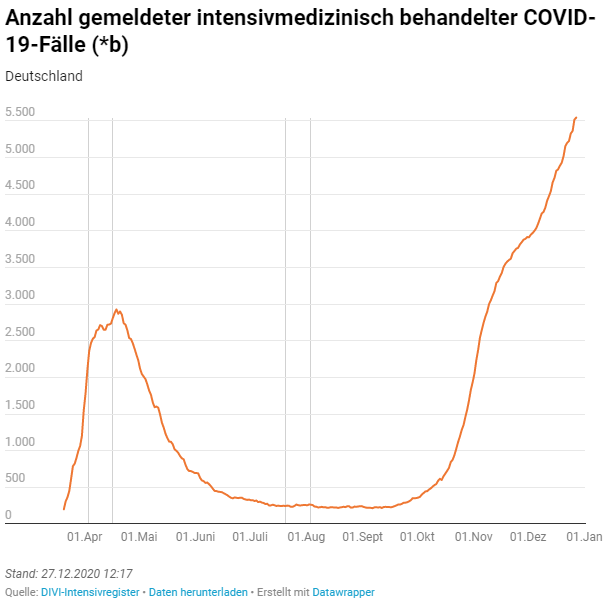
A few graphs showing current ICU usage in Germany, fitting in right with the capacity discussion above:
First, the number of Covid-19 cases in a German ICU, over time. It is pretty self explanatory even if you don’t know German:
Then, you see the number of ICU beds as reported by the hospitals. Note that the sharp rise at the beginning was because the register this data is from only started operating as the pandemic begun, and depends on hospitals manually reporting their capacity to intensivregister.de every day.
On the X-Axis is the number of beds. Dark blue are beds that are in use/occupied, light blue are free beds and green-grey is a (hypothetical) emergency capacity, often in the form of spare ventilators and monitors that could be hooked up to the bed of a normal ward, to transform it into an ICU bed. For example, Our hospital planned to transform two large parts of the operating theatre area into an adhoc ICU in case we got overwhelmed.

At last, and most interesting, you see the number of occupied beds in dark blue again, with the percentage of Covid-19 patients highlighted in dark orange:

I think this shows that, on one hand, we have plenty of ICU capacity, but on the other we also seem to need it for a lot of non-Covid related cases: Sepsis, major trauma, intracerebral haemorrhage, heart failure etc. All these things persist even through a pandemic, of course (note that I have argued almost from the start that all Covid-19 ICU cases are basically cases of viral sepsis)
edited for formatting
*edited again to give the source website: https://www.intensivregister.de/#/aktuelle-lage/zeitreihen , there you can also see these graphs for individual German states






