
That’s an excellent article you posted above, johnh. Very informative.
He estimates 1000 viral particles may be needed, but adds this is still to be experimentally determined.
For those interested in how the virus propagates, this is essential reading:
Seems like he know what he is talking about. But his angle is wrong. It’s not about how not to become infected, it’s about how not to infect others. You cannot control what others do, only what you do yourself. You can be infected by every person around you, and you have no control of a single one of them. You can infect every person around you, but you are in total control, and can chose to minimize that risk.
Let’s say only 50% give a damn about infecting others. We have still reduced the “R” from 3 to 1.5. if 2/3 give a dam, it’s already below 1. It’s an attitude and awareness among the people that is needed.
Distance, 1 m or whatever, hygiene – wash or desinfect hands periodically, and stay at home when feeling sick. That’s all it takes.
I just came back from the hair dresser. No masks, no gloves, business as usual and no Corona. And we got R down from 3.1 to less than 1/2 in about a month
Johnh – it is indeed an interesting article, but not supported by very much science (or at least the science isnt referred to).
In order to get infected you need to get exposed to an infectious dose of the virus; the estimate is that you need about ~1000 SARS-CoV2 viral particles for an infection to take hold, but this still needs to be determined experimentally. That could be 1000 viral particles you receive in one breath or from one eye-rub, or 100 viral particles inhaled with each breath over 10 breaths, or 10 viral particles with 100 breaths. Each of these situations can lead to an infection
For example, all very well – “but this still needs to be determined experimentally” – well any of us could write and guess as much. It doesnt mean anything. Why estimate a 1,000 viral particles? Perhaps there is some scientific basis for doing so?
The rest of the article is in a similiar vein. One moment it suggests that a sneeze outdoors could leave enough aerosol to reach the threshold, the next, it suggests almost all infections occur in more confined space.
As I said earlier, I have a feeling the controlled experiments havent been done, and we dont actually know how many particles it takes. I am not even convinced it is as infectious as some might believe, certainly in terms of the micro levels required for Sarin deriviatives.
That does mean I suggest it isnt highly contageous, but in terms of how the sustained amount required to infect someone, I think those that might think in terms of biologically very small amounts, I suspect it is something a bit more than that. Of course, I have no idea what the actual quantity is, and the extent to which enviromental factors might be a play.
My understanding is that it is probabilistic – a single viral particle can be enough to cause an infection, but more often it will be inactivated by the body’s defences before it does so. If you are exposed to 1000 or 10000 particles the chances of one getting through become much larger.
The ‘infectious dose’ probably applies to the dose that will cause infection in 50% of people.
we dont actually know how many particles it takes
We don’t know how many particles but we do know this thing is incredibly infectious. There have been so many documented cases where 1 person infected so many others just by being in some proximity. It is spreading around the world at a great speed and is now doing the Amazon jungle tribes.
For example, if you are working in the miasma of a COVID ward in London, the risks are worth considering, particularly if you are black or Middle Eastern and approaching retirement age. I think these people are genuinely brave.
You are brave just by being male  There is a 1.5 factor already. Being in the BAME group adds a further similar multiple (when adjusted for known conditions, apparently).
There is a 1.5 factor already. Being in the BAME group adds a further similar multiple (when adjusted for known conditions, apparently).
Let’s say only 50% give a damn about infecting others. We have still reduced the “R” from 3 to 1.5. if 2/3 give a dam, it’s already below 1. It’s an attitude and awareness among the people that is needed.
Maybe Norwegians are socially responsible, or just eat so much garlic that social distancing is automatic Yesterday there was a street party in our village (VE Day anniversary, I am told ) and when I came back from my walk I walked through it and they looked at me like I was being a bit antisocial, not stopping to have a drink with them. I think for every person who doesn’t want to catch it, there is another who is in the “live and let live” category. Then we wonder why the deaths here are not going down as fast as they ought to be
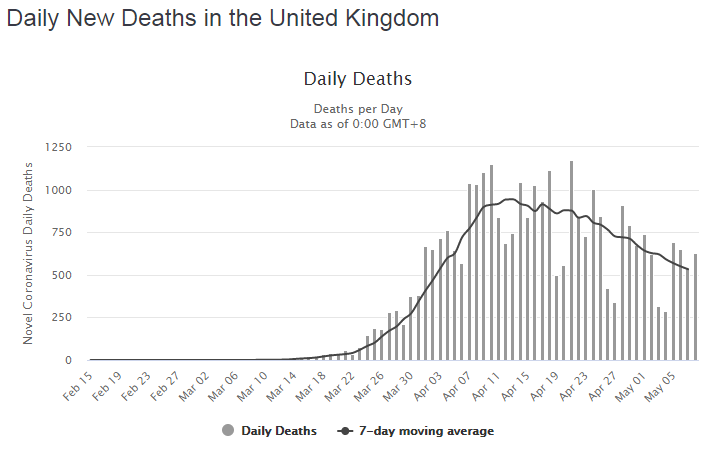
Admittedly the numbers now include care homes which probably make up about 1/3 to 1/2 of the total and they are increasing.
Peter wrote:
Maybe Norwegians are socially responsible, or just eat so much garlic that social distancing is automatic
If everybody eat garlic, then … It’s exactly the same social thing that happened with smoking. Suddenly smoking became socially unacceptable. Look at the numbers. We have had nothing of this “lockdown” (not thinking about closed airspace and a couple of other things that no one really understand, and it affected only a small number of people anyway). Shops, supermarkets, restaurants etc have been open. The big thing was closing of schools. In hindsight all evidence point towards this had no effect. It may even have worsen the “R” due to the way children behave. It certainly has worsened life for a lot of people, children, parents and their jobs, all for nothing.
Restrictions against social gathering (how many can gather together) and keeping distance has stopped the whole “social scene”, sort of, at least city life (bars, theaters, movies and similar). And there you have a point. A typical thing about Norway is you can take a trip to Oslo, or any other big city during a Sunday, and you will find the city deserted. There is no one there. Then take the same trip in the nature surrounding the city, and it’s crowded. That’s what we do on Sundays. We are either inside our homes, or we are out, skiing, hiking, cycling or simply taking a walk in nature. It is rather peculiar phenomenon. You can walk in the city, and try to say hello to someone, and they will give you a surprised and odd look back. Do the same out in the woods on a Sunday, and you will find everybody say hello to each other. What happened when Covid 19 came, was simply more outdoor activity. The last months this hammock-thing has been one of this weird thing that has happened. People (kids and young people mostly), walking out in the woods in the evening, sleeping in the hammocks during the night, partying and having a great time.
The only point now is that until a vaccine/medicine, we have to live with Corona. This means we have to stop doing the things that spread the disease, and do more of the things that have no effect on the spreading. Had a training flight today (in very windy conditions), have to be prepared, because on monday I can start instructing again
I wonder whether the differences in the way the virus has spread in different countries does indeed correlate with the tendency of the population to do outdoor activities.
In the UK, you get a predominantly urban high density living / leisure pursuits, and – as a generalisation obviously – it is the older and more wealthy people who value the outdoors, and spend the extra money on property outside cities.
LeSving wrote:
We have had nothing of this “lockdown” (not thinking about closed airspace and a couple of other things that no one really understand, and it affected only a small number of people anyway). Shops, supermarkets, restaurants etc have been open. The big thing was closing of schools. In hindsight all evidence point towards this had no effect. It may even have worsen the “R” due to the way children behave. It certainly has worsened life for a lot of people, children, parents and their jobs, all for nothing.
So apart from closing schools, the VFR ban — both of which, I agree, likely had no effect — and the border closure — which I don’t think had any effect either — Norway seems to have done the same things as Sweden.
So why are Sweden’s figures so much worse? I can think of a couple of reasons. Norway may have imposed measures earlier in their spread of the virus. The care home situation could be better in Norway. Norway didn’t have as many people skiing in the Alps.
But there must be more differences as consumer spending in Sweden has decreased much less than consumer spending in Norway.
Jersey_Flyer wrote:
Our infections have gone to zero. It makes you wonder how many of of the oppressive UK rules were needed
That’s great to hear, but I don’t think you can compare Jersey to, say, central London. This is really part of the problem. One size does not fit all. That said, it’s easy to implement a different strategy on a small island. Doing the same thing in areas that are mutually easily accessible will prob90 mean that people in the harder hit area move/travel to the one that’s opening up asnd thus spread the virus.
Peter wrote:
wonder whether the differences in the way the virus has spread in different countries does indeed correlate with the tendency of the population to do outdoor activities.
I would say definitely yes. Look at the difference between NYC (cooped up with little sunlight) and California – loads of sun, outdoors lifestyle.
Look at the difference between NYC (cooped up with little sunlight) and California – loads of sun, outdoors lifestyle.
The “political” problem, of course, is that NYC also has a lot of poorer people than California, and “social deprivation” correlates heavily with co-morbidities. But social deprivation also correlates heavily with high density living.
OTOH it is obvious that lower density living is alone capable of reducing virus spread. If you have enough of this factor, you don’t need anything else.
The BAME community also correlates heavily with social deprivation (and also with co-morbidities), but according to some recent analysis that doesn’t wholly explain the higher death rate. It explains roughly half of the excess. The rest is presumably something genetic and not yet known. But CV19 is not well understood anyway. It does things to the body which baffle doctors.
I am sure statisticians will be unravelling these factors for many years to come.




